**The McMurray Test is a cornerstone in diagnosing knee injuries, particularly those involving the meniscus. If you've ever experienced persistent knee pain, a nagging click, or a sudden locking sensation, chances are your doctor might perform this specific physical examination. It's a fundamental diagnostic tool that helps healthcare professionals pinpoint the source of discomfort and determine if a meniscal tear is the culprit behind your symptoms.** Understanding the intricacies of your knee pain can be a daunting task, but specialized tests like the McMurray Test offer crucial insights. This widely recognized orthopedic examination allows clinicians to assess the health of your knee joint and detect potential issues, guiding you towards the most appropriate treatment. Let's delve into the mechanics, history, and significance of this vital diagnostic procedure.
Understanding the Knee's Vital Shock Absorbers: The Meniscus
Before we dive deep into the **McMurray Test**, it's essential to understand the star of the show: the meniscus. Imagine your knee joint as a complex hinge, constantly bearing the brunt of your body weight and absorbing impact from every step, jump, and turn. Within this joint, nestled between your thigh bone (femur) and shin bone (tibia), are two crescent-shaped pieces of cartilage called menisci (plural of meniscus). You have one on the inner side of your knee, known as the medial meniscus, and another on the outer side, called the lateral meniscus. These remarkable structures aren't just passive cushions; they are vital for the smooth, stable, and pain-free functioning of your knee. Their primary roles include acting as shock absorbers, distributing weight evenly across the joint, enhancing joint stability by improving the fit between the bones, and contributing to the lubrication and nutrition of the knee cartilage. Without healthy menisci, the forces on your knee would be concentrated, leading to premature wear and tear of the articular cartilage, and ultimately, conditions like osteoarthritis. Meniscal tears are incredibly common, often occurring during activities that involve twisting the knee, especially when the foot is planted, such as during sports or even a simple misstep. Understanding their function helps appreciate why diagnosing their injury, often through tests like the **McMurray Test**, is so critical.
The Legacy of Thomas Porter McMurray: A Pioneer in Orthopedics
Every significant medical advancement often traces its roots back to the innovative mind of a dedicated professional. The **McMurray Test** is no exception, owing its existence to the pioneering work of Thomas Porter McMurray. Born in 1887 in Liverpool, England, McMurray was a distinguished British orthopedic surgeon whose contributions profoundly shaped the field of orthopedics. He dedicated his career to understanding and treating musculoskeletal conditions, particularly those affecting the lower limbs. McMurray's keen observational skills and deep understanding of knee biomechanics led him to develop this now-iconic diagnostic technique. He first described the test in the early 20th century, specifically designing it to diagnose posterior horn lesions of the medial meniscus – a common and often challenging injury to identify clinically at the time. In an era before advanced imaging like MRI became commonplace, physical examination was the cornerstone of diagnosis. McMurray's ingenuity provided a systematic, reproducible method to assess meniscal integrity, allowing clinicians to gain crucial insights into knee injuries without invasive procedures. His work laid the groundwork for countless diagnoses, guiding treatment plans, and ultimately improving the lives of patients suffering from debilitating knee pain. The enduring relevance of the **McMurray Test** today stands as a testament to his profound and lasting legacy in orthopedic medicine.
What Exactly is the McMurray Test?
At its core, the **McMurray Test** is a physical examination technique meticulously designed to detect meniscal tears within the knee joint. It's not a machine, a scan, or a complex laboratory analysis; rather, it's an artful manipulation of the knee by a trained healthcare professional, performed right in the examination room. This test is a series of specific knee and leg movements that can help a doctor diagnose a torn meniscus, often without the need for immediate, more expensive imaging. The fundamental principle behind the **McMurray Test** is to recreate the conditions that might cause a torn piece of meniscus to "catch" or "click" within the knee joint. By applying specific stresses and rotations while moving the knee through its range of motion, the examiner attempts to elicit symptoms indicative of a meniscal injury. These symptoms typically include pain, a distinct snapping or clicking sound, or a sensation of locking within the joint. It's a crucial orthopedic examination used to assess knee joint health and detect potential issues, providing immediate, real-time feedback to the clinician. While seemingly simple, the precision and interpretation of the test require significant expertise, making it a valuable tool in the diagnostic arsenal for knee injuries.
How is the McMurray Test Performed? A Step-by-Step Guide
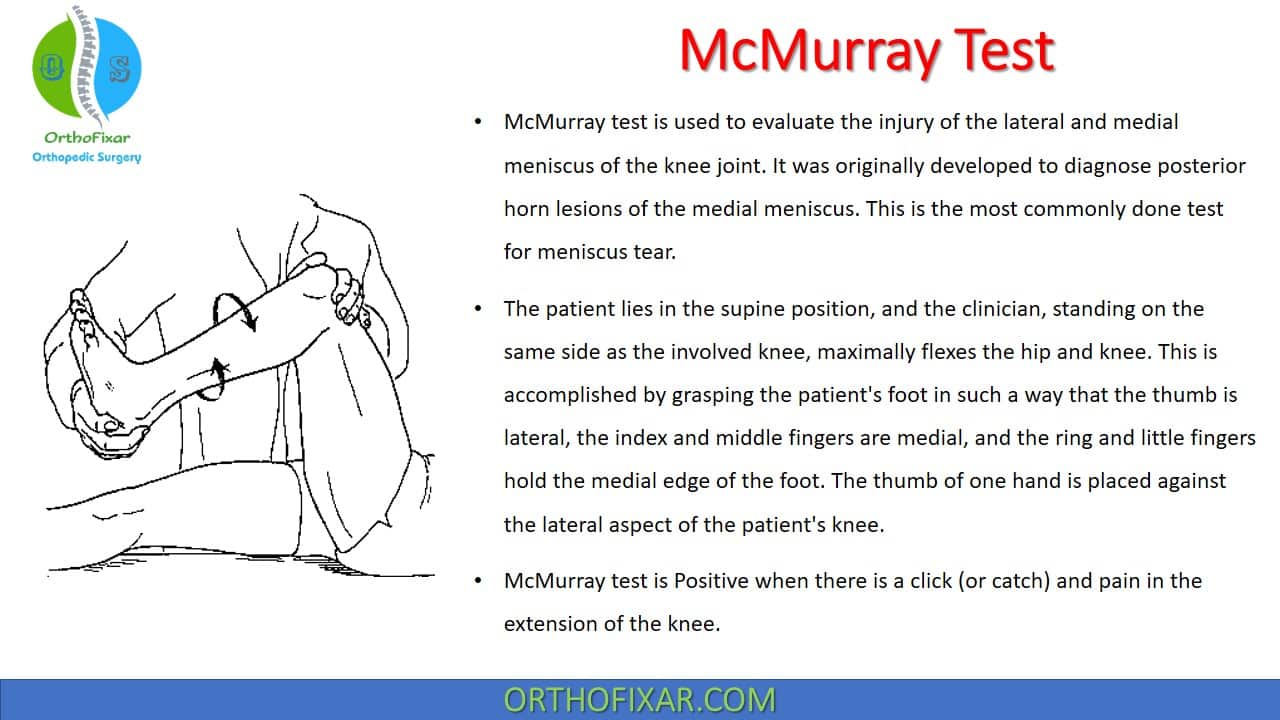
Performing the **McMurray Test** is a precise art, requiring a thorough understanding of knee anatomy and mechanics. It’s a hands-on procedure where the examiner carefully manipulates the patient's knee to provoke symptoms if a meniscal tear is present. The goal is to trap a potentially torn piece of meniscus between the femur and tibia, causing pain or a characteristic "click" or "snap."
Preparing for the Test: Patient and Examiner Positioning
The patient typically lies on their back (supine) on an examination table. The examiner stands beside the affected knee. The first step involves fully flexing the patient's knee, bringing the heel close to the buttocks. The examiner uses one hand to grasp the patient's heel or foot, providing control over the lower leg's rotation. The other hand is placed on the knee joint, specifically palpating the joint line – the space between the femur and tibia – where the menisci reside. This hand is crucial for feeling any clicks, snaps, or crepitus, and for applying the necessary varus or valgus stress. This initial positioning is key to ensuring the knee is in a state where the menisci are under tension, allowing for effective assessment.
Assessing the Medial Meniscus
To assess the medial meniscus (the inner meniscus), the examiner starts with the knee fully flexed. While maintaining this flexion, the examiner externally rotates the tibia (turns the foot outwards) and applies a valgus stress (a force that pushes the knee inwards, towards the midline of the body). With these forces applied, the examiner slowly extends the knee. The purpose of the external rotation and valgus stress is to put tension on the medial meniscus, making it more likely that a torn fragment will be impinged or "caught" as the knee moves through its range of motion. A positive finding for a medial meniscal tear would be the reproduction of pain, a palpable or audible click, or a locking sensation during this specific maneuver, particularly as the knee approaches full extension.
Assessing the Lateral Meniscus
Conversely, to assess the lateral meniscus (the outer meniscus), the procedure is similar but with opposite rotations and stresses. Starting again with the knee fully flexed, the examiner internally rotates the tibia (turns the foot inwards) and applies a varus stress (a force that pushes the knee outwards, away from the midline of the body). Just as with the medial meniscus assessment, the examiner then slowly extends the knee while maintaining these forces. The internal rotation and varus stress are designed to put tension on the lateral meniscus. If a tear is present, this maneuver can cause a torn piece of the lateral meniscus to become trapped between the bones. A positive **McMurray Test** for the lateral meniscus would manifest as pain, a click, or a locking sensation, often occurring as the knee is extended.
Interpreting the Signs: What a Positive Test Means
The interpretation of the **McMurray Test** is critical. A "positive" test result is indicated by the reproduction of the patient's symptoms, such as sharp pain, a distinct snapping or clicking sound (which can sometimes be felt by the examiner's hand on the joint line), or a sensation of the knee "locking" or giving way. The location of the pain and the specific maneuver that elicits the symptom can help the clinician determine which meniscus is involved (medial or lateral) and even suggest the location of the tear (e.g., posterior horn lesions, which the test was originally developed to diagnose). It's important to note that while a positive test strongly suggests a meniscal tear, it's part of a broader clinical picture. Conversely, a negative test doesn't entirely rule out a tear, as some tears may not be provoked by this specific maneuver.
Why is the McMurray Test So Widely Used? Its Diagnostic Value
The **McMurray Test** holds a prominent position as the most common orthopedic special test utilized in the physical diagnosis of meniscus lesions. Its widespread adoption isn't accidental; it stems from a combination of practical advantages and its undeniable diagnostic utility. One of its key strengths is its simplicity and accessibility. Unlike advanced imaging techniques that require specialized equipment and facilities, the McMurray Test can be performed in virtually any clinical setting – a doctor's office, an emergency room, or even on the sidelines of a sporting event – without the need for special machinery or extensive preparation. This makes it an invaluable first-line assessment tool for knee injuries. Furthermore, the test provides immediate feedback. Within minutes, a skilled clinician can gain crucial insights into the potential presence of a meniscal tear, guiding the subsequent steps in the diagnostic process. This efficiency is particularly beneficial when dealing with acute knee injuries where prompt assessment is vital. While diagnosis can be suspected clinically with joint line tenderness and a positive **McMurray Test**, it forms a critical part of the initial clinical picture. It helps the doctor formulate a strong clinical suspicion, which can then be confirmed with more definitive studies like MRI. The test’s ability to pinpoint the affected meniscus (medial or lateral) and sometimes even the likely location of the tear (e.g., posterior horn) further enhances its diagnostic value, making it an indispensable part of any comprehensive knee examination.
The Science Behind the McMurray Test: Sensitivity and Specificity
In the realm of medical diagnostics, tests are often evaluated based on their sensitivity and specificity – two critical parameters that describe their accuracy. The **McMurray Test**, like any clinical examination technique, has been rigorously studied to understand its diagnostic capabilities. Sensitivity refers to a test's ability to correctly identify those with the condition (true positives). If a test has high sensitivity, it means it's good at picking up actual cases of meniscal tears, so a negative result is often very reassuring. Specificity, on the other hand, refers to a test's ability to correctly identify those without the condition (true negatives). A highly specific test means that a positive result is very likely to indicate the presence of a meniscal tear, minimizing false positives. Background clinical tests used for the detection of meniscal tears provide varying levels of diagnostic parameters, including sensitivity and specificity. For the **McMurray Test**, studies have shown a range of values, which can vary depending on the type of tear, the chronicity of the injury, and the experience of the examiner. Generally, the McMurray Test is considered to have moderate to good sensitivity and specificity for meniscal tears. For instance, some studies suggest a sensitivity range of 50-70% and specificity of 60-80% for medial meniscal tears, and slightly lower for lateral meniscal tears. This variability means that while a positive **McMurray Test** is a strong indicator, it's not foolproof. It's a valuable screening tool that helps narrow down the possibilities, but it's rarely used in isolation for a definitive diagnosis. Its true strength lies in its role as part of a comprehensive clinical evaluation, guiding the need for further, more conclusive imaging studies.
When the McMurray Test Isn't Enough: Complementary Diagnostics
While the **McMurray Test** is an invaluable tool in the initial assessment of knee injuries, particularly suspected meniscal tears, it's rarely the sole determinant for a definitive diagnosis. As discussed, its sensitivity and specificity, while good, are not perfect. There are instances where a meniscal tear might be present but the test yields a negative result (a false negative), or conversely, a positive result might occur without a significant tear (a false positive). Therefore, clinicians often rely on a combination of findings and other diagnostic methods to confirm their suspicions. One common clinical finding that often accompanies a positive **McMurray Test** is joint line tenderness. This involves direct palpation along the joint line where the meniscus sits; if pressing on this area elicits pain, it further supports the likelihood of a meniscal injury. Other orthopedic special tests are also frequently performed alongside the McMurray Test to gather more information. For example, the Apley Compression Test (also known as the Apley grind test) is another common maneuver used to assess meniscal integrity, often complementing the findings of the McMurray Test. This test involves compressing the knee while rotating the tibia, attempting to reproduce symptoms. However, for definitive confirmation of a meniscal tear, especially when surgical intervention is being considered, advanced imaging studies are typically required. Magnetic Resonance Imaging (MRI) is the gold standard for visualizing soft tissue structures within the knee, including the menisci. MRI studies can provide detailed images of the tear's location, size, and type, offering a comprehensive picture that the physical examination alone cannot. In some complex cases, or when a clear diagnosis remains elusive, arthroscopic examination may be performed. This minimally invasive surgical procedure allows surgeons to directly visualize the inside of the knee joint with a small camera, providing the most accurate assessment of joint damage and enabling immediate repair if necessary. With the use of arthroscopic examination, surgeons can prove and refine clinical tests for joint damage, constantly improving our understanding of knee pathologies.
Living with a Meniscal Tear: What Comes Next?
Receiving a diagnosis of a meniscal tear, potentially after a positive **McMurray Test** and subsequent confirmation via MRI, can be unsettling. However, it's important to remember that meniscal tears are very common, and effective treatment options are available. What comes next largely depends on several factors: the type, size, and location of the tear, your age, activity level, and overall health, and the severity of your symptoms. For many smaller, stable tears, especially those in the outer, blood-supplied (red-red zone) portion of the meniscus, conservative management is often the first line of treatment. This typically involves rest, ice, compression, and elevation (RICE protocol), pain management with anti-inflammatory medications, and a structured physical therapy program. Physical therapy plays a crucial role in restoring knee strength, flexibility, and range of motion, helping to stabilize the joint and reduce symptoms. The goal is often to allow the tear to heal naturally or for the knee to adapt to the tear without surgical intervention. However, for larger tears, tears in the inner, avascular (white-white zone) portion of the meniscus, or tears that cause persistent locking, catching, or severe pain, surgical intervention may be necessary. The most common surgical procedure is arthroscopic knee surgery, which is minimally invasive. During this procedure, the surgeon can either repair the torn meniscus (meniscal repair) or remove the damaged portion (partial meniscectomy). The choice between repair and removal depends on the tear's characteristics and the potential for healing. Recovery from surgery also involves a period of rehabilitation, often guided by a physical therapist, to regain full function. Early diagnosis, often initiated by a positive **McMurray Test**, is key to determining the most appropriate and effective treatment pathway, ultimately helping you get back to your daily activities with reduced pain and improved knee function.
Conclusion
The **McMurray Test** stands as a testament to the power of clinical observation and skilled physical examination in diagnosing complex orthopedic conditions. From its origins with British orthopedic surgeon Thomas Porter McMurray, it has evolved into the most common and crucial orthopedic special test for identifying meniscal tears in the knee. By meticulously extending and rotating the knee with specific stresses, healthcare professionals can effectively assess the medial and lateral meniscus for tears, looking for tell-tale signs like pain, snapping, clicking, or locking symptoms. While the **McMurray Test** provides invaluable immediate insights and helps form a strong clinical suspicion, it's important to remember it's one piece of a larger diagnostic puzzle. Its diagnostic accuracy, including sensitivity and specificity, varies, highlighting the need for complementary tests like the Apley Compression Test and, most importantly, confirmation through advanced imaging like MRI studies. Ultimately, understanding the **McMurray Test** empowers patients to engage more fully in their diagnostic journey. If you're experiencing persistent knee pain or suspect a meniscal injury, don't hesitate to consult a healthcare professional. Early diagnosis, often initiated by a thorough physical examination including the McMurray Test, is paramount for guiding effective treatment and ensuring the long-term health of your knees. Have you ever had a **McMurray Test**? Share your experiences in the comments below! If you found this article helpful, please consider sharing it with others who might benefit from understanding this important diagnostic tool.
Mcmurray Test



{kind=link}